Search
Search
14 Search Results:
New study shows technology could play an important role in mental health support
In a study published in MDPI Journal, a team of researchers at Lawson Health Research Institute have shown that the use of technology may assist in better outcomes for those living with both mental health and physical disorders.
Dr. Cheryl Forchuk, Assistant Scientific Director at Lawson, and her team embarked on a pilot study that used smart home monitoring solutions to assist those living with both a mental health disorder and other health challenges. The purpose of this pilot study was to see if technology could improve overall lifestyle and wellbeing.
“We began our research by using hospital prototype apartments – apartment style care spaces within hospital settings – that were equipped with smart home technology solutions such as a screen device, activity trackers, weigh scales and medication dispensers,” says Dr. Forchuk who is also the Beryl and Richard Ivey Research Chair in Aging, Mental Health, Rehabilitation and Recovery at St. Joseph’s Health care London. “Once we tested it in a hospital setting, we wanted to find a way to take this idea out into the community in different kinds of housing and living situations to see if it would be beneficial.”
The research team partnered with the Canadian Mental Health Association (CMHA) and the London and Middlesex Community Housing (LMCH) to work together to retrofit the homes of the 13 study participants.
“We worked together with the participants and their care providers to choose what combination of technology they felt would be best for them,” says Dr. Forchuk. “No matter their health condition each participant wanted to be more active and independent, with the goal of staying out of hospital.”
All smart devices were connected to the Lawson Integrated Database, which is a database that can securely collect data from multiple sources such as health devices. This allowed care providers to send reminders to participants, while also tracking usage and results.
“The key benefits we noted was that study participants started to live healthier lives,” says Jonathan Serrato, Lawson Research Associate. “Participants logged going for walks and exercising more often, as well as making healthier food choices. Those who used the medication dispensers did not miss a single dose. The touch screen devices also allowed participants to easily communicate with care providers and support networks, and access more resources.”
Following the pilot study, the research team also published a subsequent paper, as a ‘how-to guide’ for utilizing smart home technology interventions as a health care tool.
“This paper is a helpful resource that outlines implications and considerations when it comes to smart home technologies,” adds Serrato. “There are many areas we touch upon such as security, privacy and feasibility as well as hardware and software information for those who would like to take on their own similar type of smart home technology project.”
$65.75M grant positions Lawson as Canadian leader in workplace-injury research
Massive investment by the Workplace Safety and Insurance Board (WSIB) to St. Joseph’s Health Care London is largest-ever grant to transform occupational illness and injury

A “game-changer” investment of $65.75 million to Lawson Research Institute of St. Joseph’s Health Care London will transform the prevention, diagnosis and treatment of workplace injuries and illness for Ontarians.
The Workplace Safety and Insurance Board’s visionary 10-year commitment is the WSIB's largest-ever research injection; the largest non-government health research funding in London history; and the biggest single grant received and stewarded by St. Joseph’s Health Care Foundation.
The investment will launch the Occupational Injury Prevention and Treatment Research Network – a first-in-Canada hub where people, technology and science-backed innovation will help solve the human and health costs of occupational injury and illness across Ontario and around the world.
Landmark work, global leadership
“This is a game-changer, something that will transform how we work together to get ahead of work-related injury, pain and mental illness,” says Lisa Porter, PhD, Vice-President Research at St. Joseph’s and Scientific director of Lawson, the research arm of St. Joseph's.
“This investment will propel us to global leadership in finding solutions to some of the most pervasive issues affecting people in workplaces today,” Porter says.
Occupational injuries and illnesses – including chronic pain, physical disability and mental health conditions – accounted for more than 93,000 claims registered through the WSIB last year, with an average lost work time of 63.2 days.
Occupational injuries and illnesses – including chronic pain, physical disability and mental health conditions – have a significant impact on many people, families and businesses in Ontario. Every year they account for almost 250,000 claims registered through the WSIB, with benefit payments of approx. $2.5 billion.
“Too many Ontario families experience the human cost of workplace injury,” says Jeffery Lang, President and CEO of the WSIB. “We want fewer injuries to happen, and if they do, to be able to help people with a safe and faster recovery. This research is going to help get us there and with their established expertise, the St. Joseph’s Health Care and Lawson Research Institute team are a natural partner for this important work.”
Investment and innovation
The network will innovate long-term solutions to prevent mental and physical injuries, accelerate recovery and ensure sustainable health for Ontario workers.
It will feature state-of-the-art infrastructure and expertise including:
- A first-in-Canada positron emission tomography/magnetic resonance imagery (PET/MRI) scanner dedicated to research into rapid and accurate diagnosis of mental health conditions including post-traumatic stress and depression
- A cutting-edge Computer-Assisted Rehabilitation Environment (CAREN), a unique, virtual-reality environment that will test and solve workplace injury, rehabilitation and chronic pain in new ways
- Three new endowed research Chairs and teams of scientists solving the most critical research questions plaguing people injured at work, an investment that will ensure long-term consistency and sustainability of the work
- Deploying technology in data science, artificial intelligence (AI) and virtual reality, making the network accessible by centres and workplaces across Canada
Rapid-access research area to design and test assistive devices such as splints and mobility technology
St. Joseph’s President and CEO Roy Butler says, “We know that discovery-driven, patient-focused research improves lives – that is the focus of our hospital-based research at Lawson, and we’re humbled that the WSIB has entrusted us to expand this vital work to minimize the effects of workplace injury, disease and disability. This significant investment will drive innovation opportunities that will translate into novel new treatments and tools that can be used to battle workplace injury and illness”
“This investment will enable us to leverage the deep expertise St. Joseph’s already has in mental health, chronic pain and rehabilitation, and creates the opportunity to expand our knowledge to support workplace wellness, including for frontline health-care workers,” Butler says.
Butler adds that the network will strengthen existing partnerships and create new collaborations – within St. Joseph’s as well as among a wide range of health professionals, researchers, post-secondary institutions and industry locally, across the province and nationally.
Butler notes St. Joseph’s already excels in research and treatment for related injuries and illnesses.
That includes: preventing and treating chronic pain through the hospital’s Pain Management Program and the Gray Centre for Mobility and Activity hand and upper limb care and injury prevention through the Roth | McFarlane Hand and Upper Limb Centre; advanced imaging expertise; and mental health solutions for veterans and first responders at the MacDonald-Franklin OSI Research Centre. All are specialty research areas of St. Joseph’s with deep roots in addressing occupational injury and illness.
A partnership of promise

Many groundbreaking research initiatives at St. Joseph’s have been made possible by generous supporters of St. Joseph’s, says Michelle Campbell, President and CEO of St. Joseph’s Health Care Foundation.
Medical research in Canada, including the research done in our hospitals, relies heavily on private funding. Donors to our foundation, invest in research because they know that innovation leads to better frontline care, and healthier communities,” Campbell says.
“It’s a partnership of promise, a confident stride toward better outcomes for patients. The WSIB’s gift through St. Joseph’s Health Care Foundation is a whole new level of leadership, and we’re proud to be integral to this transformation in workplace health,” says Campbell.
Earlier this year, the WSIB announced a $20-million gift to Fanshawe College to create a Centre of Excellence in Immersive Technology for Workplace Safety, primarily to help first responders and responders-in-training learn to prevent and treat occupation-related mental health issues such as PTSD, anxiety and depression.
The Network at St. Joseph’s broadens that work to bring research-specific innovation aimed at benefiting the physical and mental wellbeing and safety of workers in all occupations.
The new hub at St. Joseph's will make use of the institution’s vast community and research partnerships throughout London and across Canada, in multiple collaborations across a wide range of health disciplines.
Assessing neurofeedback in stroke survivors
Researchers are testing whether a specialized form of imaging can help in stroke rehab.
A new study aims to assess the use of functional near-infrared spectroscopy (fNIRS), a type of imaging, to provide neurofeedback during stroke rehabilitation with a goal of eventually improving patient outcomes.
fNIRS is used to detect changes in brain oxygen levels using light. More recently it has also been used to develop brain-computer interfaces (BCIs), which allow patients with brain injuries to control devices like robotic arms with their thoughts.
Dr. Sue Peters, a Scientist at Lawson Health Research Institute and Director of the Neurorehabilitation Physiology Lab at St. Joseph Health Care London’s Parkwood Institute, was one of the recipients of the Spring 2022 Lawson Internal Research Fund (IRF) Awards.
The funds will go towards a new study to assess whether fNIRS can be used to direct neurofeedback in stroke survivors – helping them with rehabilitation.
“Currently, there's no real measure of brain activity that is used in stroke rehabilitation to help make clinical decisions,” says Dr. Peters, who is also a Professor at Western University.

Over 400,000 Canadians live with the effects of a stroke, according to the Heart and Stroke Foundation, and there’s hope that fNIRS could make a big difference by eventually improving movement and independence.
“We're going to use the device in some common tasks that people might do with their arm and determine whether we can use this device reliably and accurately in a stroke-related context,” Dr. Peters explains.
Participants in the study will imagine moving while remaining still. This activates very similar parts of the brain to when people actually move. If done correctly, patients will see a visual cue generated through measurement using fNIRS.
“We know from MRI studies that when I move my right hand, the left side of my brain is activated,” notes Dr. Peters. “We think we can use this concept in stroke rehab.”
Dr. Peters is recruiting 40 people from the community who are at least six months post stroke and 40 healthy adults of all ages. They will first participate in motor assessment with a physiotherapist and then wear an fNIRS cap while thinking about moving their wrist to measure brain activity.
Previously, there were a lack of methods to image the brain during real-life movement.
“The hope is to eventually conduct a clinical trial where we're testing motor interventions to see whether some things are more effective than others at activating the regions of the brain that were impacted by the stroke.”
Dr. Peters believes the study has the potential to have a big impact on the future of rehabilitation for stroke patients, leading to lasting changes in quality of life.
Celebrating Clinical Trials Day
Clinical trials are the gold standard in medical research, used to test new treatments and medical devices to ensure they are safe and improve patient outcomes.
Each year on May 20, Clinical Trials Day aims to raise awareness about the importance of clinical trials. At Lawson Health Research Institute, our researchers, research staff and learners across London Health Sciences Centre (LHSC) and St. Joseph’s Health Care London (St. Joseph’s) are working daily to advance clinical trials for some of the most pressing health challenges.
“If you look at many areas of medicine, like cancer and cardiovascular disease, part of why those conditions have had dramatic improvements in outcomes over the last several decades is because of clinical trials,” says Dr. Amit Garg, Scientist at Lawson, Lead for the Kidney, Dialysis & Transplantation Research Program at ICES Western, and a Nephrologist at LHSC.
Clinical trials can also provide patient participants with new treatment options and can demonstrate when existing treatments have applications for other diseases.
“We could not conduct clinical trials without patients participating in them,” adds Dr. David Palma, Associate Scientist at Lawson and Radiation Oncologist at LHSC. “A clinical trial is a very rigorous process where we carefully define a treatment and follow patients very closely with extra interventions and tests to see not only how the disease is responding to treatment, but also any effects on a patient’s quality of life.”
It also takes a team to make clinical trials a success, including the critical work of research coordinators, associates and assistants, adds Dr. Swati Mehta, Lawson Scientist based at St. Joseph’s Parkwood Institute.
Dr. Palma also notes that while clinical trials require investment to conduct them, they can ultimately lead to savings in the health system.
“While the primary goal of a clinical trial is to improve or save lives, they often lead to cost savings down the road. Improving cure rates means people don’t need as much treatment and that can save the initial investment many, many times over,” Palma says.
Looking ahead, work is ongoing to make clinical trials more efficient and equitable.
“Eliminating specialized infrastructure would help make trials more equitable, so they are available in smaller communities and at distant sites that otherwise would not have access. Making study materials available in multiple languages and to anyone with accessibility issues can also help,” Garg adds.
“Future clinical trials will need to follow more pragmatic, adaptive study designs that allow us to evaluate therapies or interventions in a more realistic setting,” Dr. Mehta says. “These would also allow us to follow-up with patients that were potentially underrepresented in past research.”
According to researchers at Lawson, the future of clinical trials is bright with hundreds of trials currently underway at LHSC and St. Joseph’s with the goal of improving patient outcomes.
Changing our MINDS
Local youth use art and storytelling to illustrate the personal and system challenges in mental health.
The words and images are both heartbreaking and hopeful.
“Nobody likes you if you are sad.”
you are enough. stay strong. let life surprise you.
“Please don’t leave like everyone else.”
1 year sober. 1 year of school. 1 year building a safe home. 1 year loving myself.

Zine-writing, a personal and introspective medium often used by people who have been marginalized, is an important part of local research that is finding solutions to complex mental health challenges among young adults. Its name derives from its magazine (“zine”) format.

“When we make the voices of people with lived experience central to our research, we can learn from each other and then change the system together,” says Dr. Arlene MacDougall, founder of MINDS of London-Middlesex.
The social innovation and research lab based at St. Joseph’s Health Care London (St. Joseph’s) is dedicated to designing, piloting and testing mental health innovations for teens and young adults. Its recent evolution into MINDS 2.0 adds insights by and for people up to age 35 who have complex, pervasive mental health and addiction issues.
Learning from experts
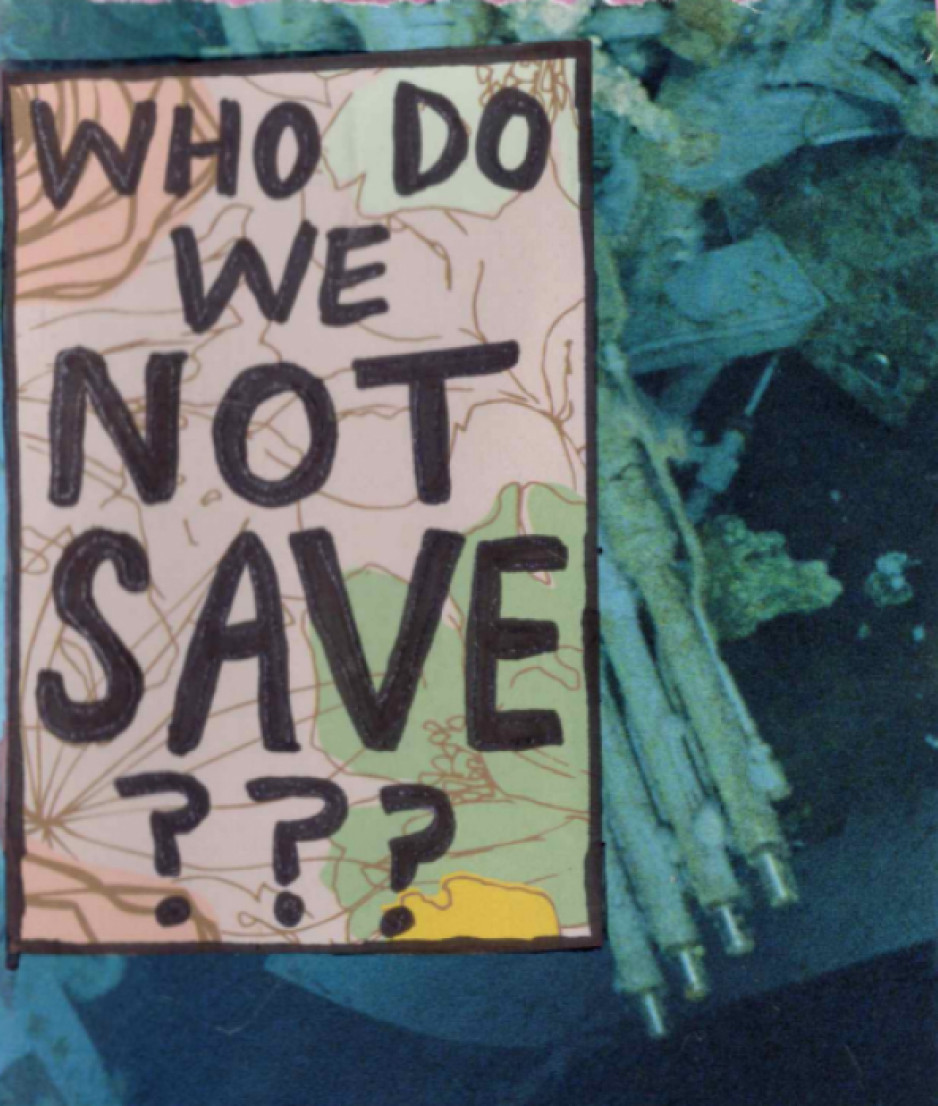
Rin, a London artist, who has published independent zines for a decade, created three for this project, including one that, with irony, asks the reader to ponder which vulnerable people aren’t worth saving.
“I believe making art can be very healing,” says Rin. “I wanted to share some of my story to help myself and help others. I want to play a part in shaping a mental health system that’s better than the one I encountered.”

The zines weave art, prose and poetry into story:
3 things I would change: affordability, stigma, waitlists.
“If I had a magic wand, I would use it to heal the waters, grow the trees, foster animal growth.”
Look in the mirror, see how far you’ve come.
They also raise and propose solutions to troubling issues among people with mental illness: housing and homelessness, sparse resources for people with addictions, lack of coordination among service providers, and dehumanizing attitudes in health and criminal justice systems.
“Participants experienced catharsis just in telling their stories,” says Renee Hunt PhD, Associate Director of Research and Operations at MINDS. “And because they’re the experts, they’re also playing an important part in changing systems that need an overhaul.”
Adds Rin, “It feels empowering knowing people are listening to us – people who care and are committed to making change to the system.”
MacDougall notes the pivotal role of St. Joseph’s Health Care Foundation – in particular, a groundbreaking $5-million donation towards mental health research from philanthropist Ryan Finch – in advancing mental health innovation through MINDS and MINDS 2.0.

“They’ve been our biggest supporters since day one. This wouldn’t have happened without support from Ryan and the foundation and all the many donors who believe in mental health research,” says MacDougall, who is also Director of Research and Innovation with St. Joseph’s Mental Health Care Program.

“MINDS has been a catalyst for system change,” MacDougall adds. “Research is always about finding answers and generating impact.”
Many findings from MINDS research have been put into practice, among them are the creation of guidebooks for peer support, free taxi service for rural youth needing urban mental health or addiction services, and educational resources to support 2SLGBTQI+ students.
MacDougall says MINDS 2.0 expands that work with new voices and the exploration of more in-depth solutions.
What’s next for MINDS 2.0
- Workshopping ideas and prototypes for mental health systems change. Sessions will be held where people with lived/living experience and service providers propose and develop potential solutions.
- Leadership-building. Twenty mental health practitioners will be trained to become “agents of change” who will collectively create, implement and evaluate mental health programs, technology, interventions and training.
- Imaginarium conference. In 2025, a first-of-its-kind national conference will take place to share system innovations in mental health and addiction.
Cyclotron hits 10,000-bombardment milestone
Cyclotron staff at St. Joseph’s Health Care London have recorded a 10,000-mark milestone in the same understated way they work every day to improve patient care and cutting-edge research.
No balloons, no streamers, no fanfare: Just an efficient note atop a printout as the bombardment number spun past 9,999 in the early hours of Dec. 31.
“It’s taken us 15 years to get to this point and our work continues to grow,” says Michael Kovacs, PhD, Lead of Lawson’s Nordal Cyclotron & PET Radiochemistry Facility and Leader of the Imaging Research Program at Lawson Research Institute, the innovation arm of St. Joseph’s.
“The numbers are great but the real satisfaction is knowing every single bombardment means something important to a patient or a researcher working towards better patient health.”

St. Joseph’s GE PETtrace cyclotron is a particle accelerator that produces radioisotopes for use in positron emission tomography (PET) scans across Southwestern Ontario, from Windsor to Toronto. It is a vital tool for ultra-precise cancer diagnoses and for advanced research into scores of diseases.
In patient care, each “bombardment” – a grouping of radioisotopes that are then lab-processed, tested and made into smaller batches – can be used to aid cancer scans for as many as 25 people.
“A precise scan can make a dramatic difference, a life-changing difference, in how someone’s cancer is diagnosed and custom-managed,” Kovacs says. “If we think of the PET scanner as the engine of that transformative work, the cyclotron’s radioisotopes are its rocket fuel.”
Isotopes injected into patients are designed to have a short radioactive half-life – between two minutes and 110 minutes – which is another reason St. Joseph’s cyclotron is such an asset for timely care in the region.
“You can’t store or stockpile them. You have to use them almost immediately, so it’s essential to local and area hospital centres to have a ready, reliable source nearby,” Kovacs says.
About half the batched bombardments are used in patients to help with clinical diagnoses that will guide doctors’ treatment decisions.
The other half are used for research trials and pre-clinical research through Lawson, in fields as diverse as oncology, cardiology, neurology, psychiatry, metabolic disease and infectious diseases. In one promising study, for example, they’re being used to image specific brain proteins as researchers explore new disease-modifying treatment pathways for Alzheimer disease.
The next burgeoning field, Kovacs says, is theranostics: the science of diagnosing cancer and precision-attacking it at the same time. “That’s exciting for me, to be able simultaneously to see what we treat and treat what we see.”
About 15 highly specialized staff work at St. Joseph’s cyclotron facility, plus PhD-candidate researchers and other trainees.
Generous donors through St. Joseph’s Health Care Foundation have made much of this advanced research and next-level technology a reality. During the past few years, the Foundation granted nearly $800,000 in donor support to fund extensive renovations to the facility, making it possible to increase production of isotopes and expand life-saving care. Recently, $1 million in donations supported a new PET/CT scanner – the heart of Canada’s first national GE centre of excellence in molecular imaging and theranostics being developed at St. Joseph’s Hospital.
“We know the cyclotron is a critical tool in our imaging work and we are grateful to those donors who stepped up to help us with renovations that enabled the doubling of our facility’s production capability,” says Michelle Campbell, President and CEO of St. Joseph’s Health Care Foundation. “This renovation helps keep St. Joseph’s imaging program at the cutting edge of clinical care.”
The 40-tonne, room-sized cyclotron is more than a machine, and more than the experts who process, test, ship and use the radioisotopes, Kovacs notes.
It’s also testament to the vision of St. Joseph’s long-time chief medical physicist Frank Prato, PhD, and to the support of hospital administrators who saw its need and potential, he adds.
“We are innovators, and our vision is that we’re going to expand St. Joseph’s imaging expertise on an even larger world stage,” Kovacs says.
Dementia research hits the ‘mark’
St. Joseph’s Health Care London is at the forefront of national research exploring biomarkers to better predict dementia and slow its onset.
Dr. Michael Borrie is now seeing grandchildren of patients who came to his clinic when he first started Alzheimer’s research 30 years ago.
His message to this new generation is more hopeful than ever, bolstered by ever-more-reliable ways of early detection and being tantalizingly close to a future of predicting dementia and intervening even before symptoms appear.
“The ultimate goal is to slow cognitive decline – and to stop it if we can – so that people can live independently, and happier, for a lot longer,” says Borrie, Medical Director of the Aging Brain and Memory Clinic at St. Joseph’s Health Care London (St. Joseph’s).
“We’re aiming to alter the trajectory of dementia,” he says.

A geriatrician, clinician and researcher, Borrie is also Platform Lead for the Comprehensive Assessment of Neurodegeneration and Dementia (COMPASS-ND), a long-term study within the Canadian Consortium on Neurodegeneration and Aging (CCNA).
Recently, the Canadian Institutes of Health Research announced $20.6 million in funding to continue the work of CCNA, a 30-site, multi-pronged project of which the St. Joseph’s-based team is the lead player. The grant will enable them to advance the frontiers of dementia research to benefit real-world patients here and across the country.
Solving mysteries with biomarkers
Despite the prevalence of Alzheimer’s and other neurodegenerative diseases – and with more than 10,000 new diagnoses in Canada each year – there are still many mysteries to solve: Why do some people have early-onset dementia while others, super-agers, remain alert and active in their 90s? What’s happening genetically, in their environment and personal medical history to advance or protect against the disease?
What is known, however, is the link between damaged nerve cells and specific proteins that misfold and clump together to form amyloid plaques and tau tangles in the brain. Detecting these abnormal proteins early is an important key to diagnosis and prediction.
Locally, the most comprehensive tool has been state-of-the-art brain Positron Emission Tomography (PET) scanning at St. Joseph’s Imaging. Lawson researchers are also involved in reliably detecting amyloid proteins by analyzing participants’ cerebrospinal fluid (CSF) – a surprisingly accurate way of confirming imaging results, says geriatrician Dr. Jaspreet Bhangu, a Lawson scientist and head of the biomarker project.
Through the BioMIND regional research project, Lawson scientists are analyzing PET scans, blood and CSF samples to check for specific protein biomarkers. If shown to be reliable, a series of these tests over time could signal whether the disease is progressing, and could predict whether it will progress or respond to treatment.
All that gets added to an arsenal that includes tests of behaviour, memory and cognitive function.
“It’s a triple assessment, or even a quadruple one, that we can conduct over time. We hope to use these advanced tests to provide vital information, similar to what is done in certain types of cancer,” Bhangu says.
But that’s not all.
Testing potential treatments
St. Joseph’s is also one of the country’s most active sites for clinical trials into whether novel medications might be able to directly pinpoint and destroy the proteins that cause Alzheimer disease.
“This is the intersection of cutting-edge research, top-notch resources and excellent clinical practice to develop personalized treatments,” says Bhangu. “What makes us unique in Canada among dementia researchers is that our science is taking us from bench to bedside – a rapid turnaround from research to direct patient benefit.”
If a person has a strong family history of Alzheimer disease and no symptoms – but does have positive biomarkers confirming presence of disease – they may then choose to take part in a randomized controlled trial to try to alter the trajectory of the disease.

“It’s still in a research context, still in clinical trials – but if Health Canada ultimately approves a treatment, we’ll have the ability and the patient database to be able to translate our findings into clinical practice much more quickly instead of waiting for years,” says Borrie.
All this is good news for a generation eager for answers, Borrie says.
“When we learn more about the mechanisms of the disease, we can find more effective, earlier treatments. And if we can treat people earlier, we hope to move the disease progression curve to the right, to add more years of good cognitive health to someone’s life.”
Detecting the Undetectable
A simple fall can lead to long-term hand problems such as arthritis due to fracturing the scaphoid bone in the wrist. Scaphoid fractures are known to have the highest rate of healing failures. While this bone’s fragile blood supply is commonly thought to be the main reason for why it is difficult to heal, Dr. Ruby Grewal is looking into a different reason – infection.
Infections are known to cause difficulty in healing bones, but traditional tests for infections in the scaphoid have come up negative. With new advancements in detecting microbial DNA, scientists can now test for ‘clinically undetectable’ infections.
Image

In a new study, Dr. Grewal will use microbial DNA test whether or not there are infections in the scaphoid fracture which causes improper healing of the bone.
“The goal of this study is to use advanced DNA sequencing technology to test whether or not we can detect evidence of microorganisms in non-healing scaphoids,” explains Dr. Grewal, Lawson Scientist and Orthopaedic Surgeon at the Roth McFarlane Hand and Upper Limb Centre (HULC) at St. Joseph’s Health Care London.
Finding new causes of improper healing of the scaphoid bone could improve treatments for individuals with these injuries and prevent long-term problems with hand function. These insights into the causes of improper healing could also prevent young patients from developing wrist arthritis.
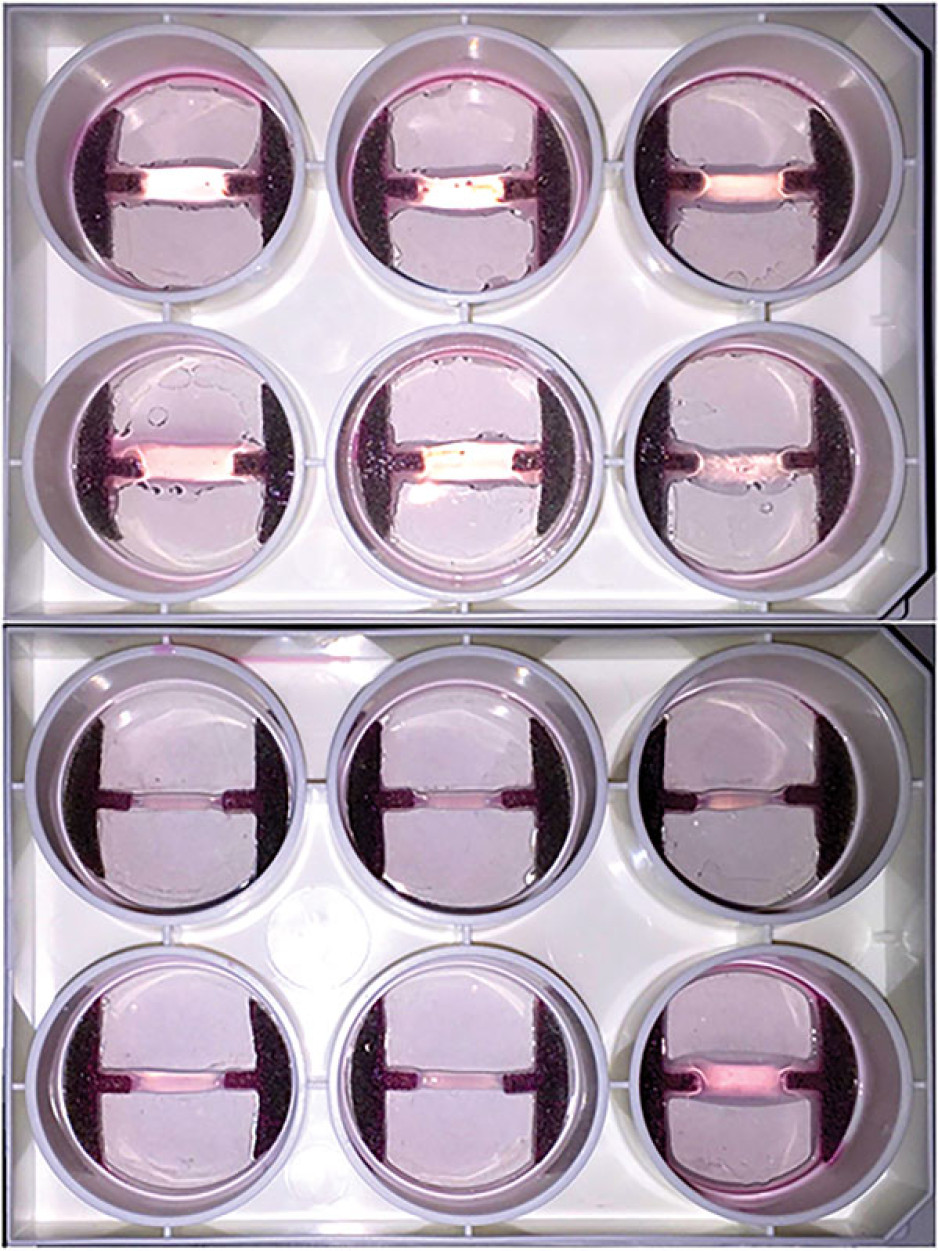
Image
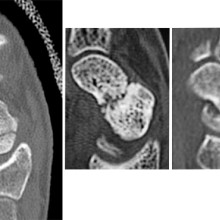
From left to right: Normal scaphoid fracture. Scaphoid fracture that is struggling to heal. Scaphoid non-union where the bone has failed to heal.
Dr. Grewal’s study is being funded through the Lawson Internal Research Fund (IRF).
“The financial support provided by Lawson’s IRF is of utmost importance to researchers. These funds will allow our team to embark on a new area of research and test a novel hypothesis,” says Dr. Grewal, “While traditional granting agencies are reluctant to fund completely novel areas of research without pilot data to prove feasibility, the Lawson IRF allows researchers to investigate new theories in a sound scientific manner. Without the ability to test new ideas we cannot innovate and make advancements in health care. Support for this project allows for that.”
Lawson’s IRF is designed to provide Lawson scientists the opportunity to obtain start-up funds for new projects with the potential to obtain larger funding, be published in a high-impact journal, or provide a clinical benefit to patients. Funding is provided by the clinical departments of London Health Sciences Centre and St. Joseph’s Health Care London, as well as the hospital foundations (London Health Sciences Foundation and St. Joseph’s Health Care Foundation).
Drug combats underlying causes of Alzheimer-related dementia
A “game-changing” new drug offers both hope and time to some people diagnosed with Alzheimer’s disease, says the head of a St. Joseph’s program that played a key role in the medication’s clinical trials. Health Canada has newly approved lecanemab (brand name Leqembi, developed by Eisai Co. and Biogen), which has been shown to slow progression of Alzheimer’s disease in people with mild symptoms.
St. Joseph’s Health Care London, and its innovation arm at Lawson Research Institute, has played a key role as one of multiple sites that have trialed the drug.
“This is game-changing,” says Dr. Michael Borrie, medical director of the Aging Brain and Memory Clinic at St. Joseph’s, whose work in dementia research and clinical practice spans more than three decades.

“We’ve been working for over 20 years to find a compound that is disease-modifying. This is the first approved drug in Canada that addresses the underlying pathology of Alzheimer’s, not just the symptoms.”
Lecanemab works by removing amyloid proteins that accumulate as sticky clumps in the brain and are associated with cognitive decline in people with Alzheimer’s. “It reverses one aspect of the disease by removing the plaque from the brain ,” Borrie explains.
“You can characterize its benefit in terms of time saved. If you were to have this medication for four years, you can ‘save’ one year of cognitive decline. It totally changes the course of their neurodegeneration in a way we haven’t seen before.”
Lecanemab was one of many clinical drug trials assigned to research coordinator Kayla Vander Ploeg when she arrived to work at St. Joseph’s more than a decade ago. “For so long, we had hope that one of these medications would benefit patients long-term. Now we have more than hope. We have results,” Vander Ploeg says.
“Today I’m seeing people who say, ‘my dad or my mom was in this study, and now there’s hope for me.’ ”
There are specific eligibility criteria, including confirmed diagnosis – through cognitive testing and through advanced brain imaging and biomarker tests – plus screening to rule out two gene variations that couldresult in more side effects.
Canada is now one of 51 countries to have approved lecanemab.
Borrie cautioned that Health Canada approval doesn’t necessarily translate to funding coverage. It’s not yet determined who will pay for the medication, or how: when lecanemab was approved in the United States in 2023, the annual cost per patient was more than $26,000.
The length of time from drug development to trials to approval illustrates how painstaking pharmaceutical research can be. But it also highlights how integrating health research into hospital settings can translate more quickly into improved patient care.
Growing Tissues in the Lab
When challenged by surgeons to find better treatments for difficult-to-manage connective tissue diseases, Dr. David O’Gorman gladly accepted.
Dr. O’Gorman is a Molecular Biologist and Lawson Scientist based at St. Joseph’s Hospital, a part of St. Joseph’s Health Care London. His research focuses on understanding normal and abnormal connective tissue repair. He collaborates with researchers and clinicians working in many different disciplines, including those specializing in reconstructive surgery, orthopedics and urology.
Surgical reconstructions can be hampered by a lack of graft tissue, or graft tissue of insufficient quality, making it difficult to achieve optimal outcomes for the patients.
An example is a condition called urethral stricture disease (urethral scarring). This condition occurs in males and typically causes symptoms such as frequent and urgent urination, and slow urinary stream. In extreme cases, it can cause urinary tract infections, permanent bladder dysfunction and renal failure. Recurrence rates after minimally invasive treatments are high, and so many urologists recommend open surgical approaches.
Surgeons can use the patient’s own tissues to reconstruct the urethra after stricture removal. This tissue is normally sourced from the buccal cavity in the mouth but taking large tissue grafts can result in complications. In cases where buccal grafts have been used for previous reconstructions, there may not be enough intact tissue left.
Dr. O’Gorman sees a solution in growing sheets of human buccal tissues in the lab.

“We are currently using buccal graft trimmings as a source of cells, culturing them in a 3D environment and expanding them to create tissues of suitable size, density and elasticity.”
The patient’s own cells are used to generate a tissue graft for urethral reconstruction. While several research groups have developed this approach in the past, few have attempted to translate their models for clinical use.
“Our immediate goal is to provide proof of principle – that we can consistently generate grafts of suitable size and functional characteristics,” explains Dr. O’Gorman, “In the future, we could be providing bioengineered graft tissues for reconstructive surgeries here in London.”
Bioengineered human tissues can also be used as ‘mimetics’ – replications of human tissues – to study diseases, especially those difficult to model using routine laboratory methods.
Instead of a using a growth media or sterile plastic dishes, 3D cell culture is achieved by embedding cells in a matrix of proteins and other molecules normally found in those tissues. In this environment, gene expression and growth is more similar to cells of connective tissues in the body being replicated.
Dupuytren’s disease (or Dupuytren’s Contracture) affects the palmar fascia in the hand, a connective tissue beneath the skin that extends from the base of the palm into the fingers. This disease can be understood as a type of excessive scarring, where normal tissue repair processes have gone awry and dense scar tissue forms, typically causing permanent palm or finger flexion that restricts hand function.
This condition is surprisingly common and may affect more than one million people in Canada. While there are surgical treatment options available, none consistently prevent this disease from recurring in at least a third of patients.
“Due to its high recurrence rate after treatment, Dupuytren’s disease is currently considered incurable. Our challenge is to understand it well enough to develop truly effective treatments,” says Dr. O’Gorman.
Human hands have unique characteristics not found in other species, making animal models impractical. Instead, Dr. O’Gorman’s team extracts cells from the diseased palmar fascia of patients undergoing hand surgeries and bioengineers them into palmar fascia ‘contractures’ in the lab.
“Since the cells from a single palmar fascia sample can be used to grow dozens of little contractures, we can test many different treatments simultaneously to see what works best for each patient.”
This approach may also allow them to determine if Dupuytren’s disease is truly one disease, or a group of similar diseases that cause palm and finger contractures.
“Often, Dupuytren’s disease is clearly heritable, but some individuals have no family history of it and develop apparently sporadic disease,” notes Dr. O’Gorman. “We want to determine if these are truly the same disease at the molecular level.”
Another major cause of abnormal connective tissue repair is infection, and tissue mimetics can play a role here, too. While rare, infections of artificial joint replacements are particularly devastating for patients, as they typically require readmission to hospital to remove the infected joint, weeks of antibiotic-based treatment, and an additional surgery to replace the artificial joint.
In addition to the associated pain and suffering, these procedures are technically challenging and costly to our health care system.

Artificial shoulder joint infections are most frequently caused by the microorganism Cutibacterium acnes (C. acnes). C. acnes infections disrupt normal tissue repair processes after surgery, cause shoulder tissues to die and promote loosening of the artificial joint. These infections are difficult to diagnose, and there is a lack of reproducible
models in which to study them. Dr O’Gorman’s team has set out to create the first human Shoulder-Joint Implant Mimetic (S-JIM) of C. acnes infection.
“While S-JIMs are more complex, they are 3D in vitro cell culture systems designed to mimic human tissues, like those that we use for studying Dupuytren’s disease.”
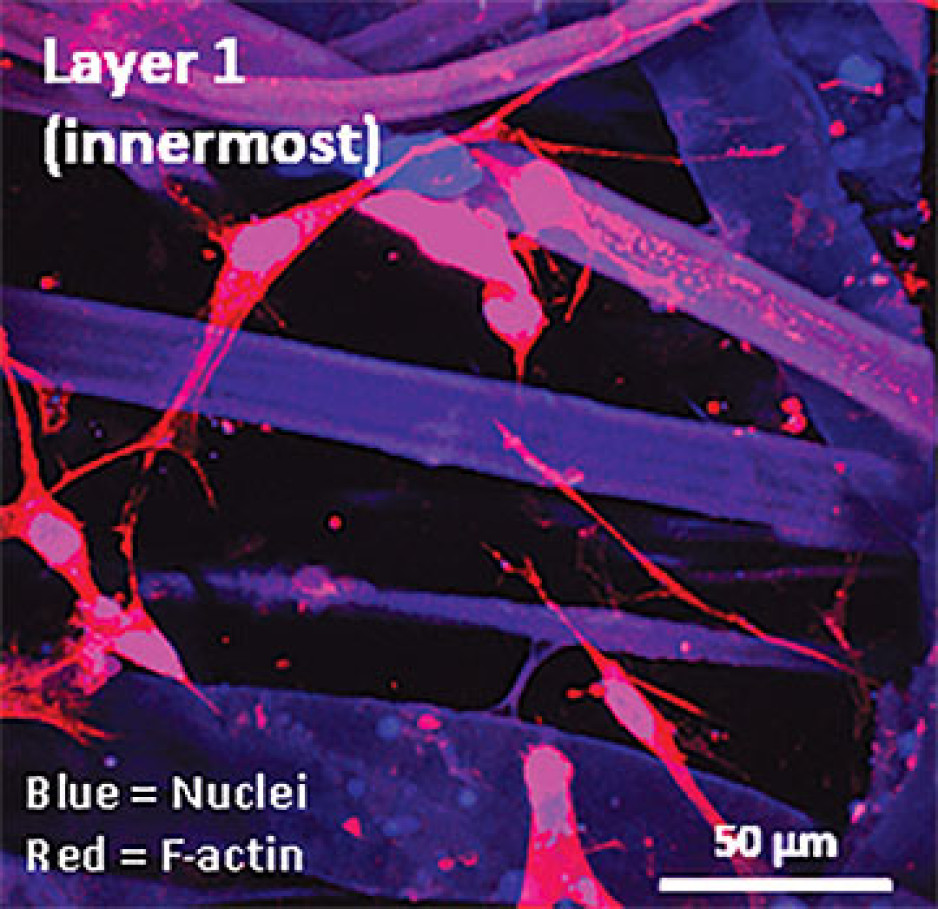
S-JIMs include layers of artificial human tissue, wrapped around cores of titanium alloy or cobalt chrome, the metals used to create artificial joints. They are co-cultured with C. acnes under low oxygen conditions similar to those that normally occur around artificial shoulder joints.
“We are bioengineering simple 3D cell cultures to more closely mimic the complexity of human tissues, with blood supply, nerves and interactions with other cells.” – Dr. David O’Gorman
Studying the connective tissue layers close to the infection allows researchers to investigate processes that promote infection, such as the formation of a biofilm that harbours and protects the bacteria from the body’s immune system. They are also able to test whether novel treatments can disrupt biofilm formation and increase the effectiveness of antibiotics.
Dr. O’Gorman predicts that in the future, medical researchers will routinely use bioengineered 3D human tissue and organ mimetics to accelerate our understanding of disease.
“The technology is in its infancy, but the potential for using bioengineered human tissues for surgical reconstructions or as disease models is huge. At Lawson, we’re ready to take on health care challenges and build on innovative approaches to improve the quality of life for patients.”
ONLINE EXCLUSIVE: What is 3D cell culture?
Medical researchers have grown human cells in culture media on or in sterile plastic dishes, such as Petri dishes, for more than 50 years.
Some cells, such as blood cells, can survive and grow in suspension, while others like smooth muscle cells need¬ to adhere to a surface to survive and grow. These are often called “2D cell cultures” because the cells grow horizontally across the bottom of the dish.
Some cells derived from connective tissues, such as fibroblasts, are not only adherent, but also very sensitive to the stiffness of their environment (“biomechanically sensitive” cells). Plastic dishes are at least 10,000 times stiffer than most connective tissues, and when biomechanically sensitive cells detect stiff surfaces, they can change the expression of their genes and behave abnormally.
The most common proteins in these tissues - and in the entire human body - are collagens, and one routine 3D cell culture approach is to embed fibroblasts in a collagen gel (gelatin). Fibroblasts in this environment can grow in any direction they choose, and their gene expression is more similar to cells in connective tissues.
These simple 3D cell cultures represent tissue engineering in its most basic form.
“Our challenge is to bioengineer simple 3D cell cultures in the lab to more closely mimic the complexity of human tissues, which have blood supply, nerves and interactions with other cells and tissues that modify their function and ability to heal after injury,” explains Dr. O’Gorman.
Dr. David O’Gorman is a Lawson Scientist and Co-director, Cell and Molecular Biology Laboratory at The Roth | McFarlane Hand and Upper Limb Centre in London, Ontario. He is also an Assistant Professor at Western University.
Maternal diabetes impacts oxygen flow in umbilical cord, study suggests
A new Lawson Health Research Institute study published in the journal Placenta has found a unexpected difference in the impact of pre-existing diabetes versus gestational diabetes on oxygen flow in the umbilical cord during pregnancy.
Currently, tests done very close to the end of a high-risk pregnancy can’t reliably measure the full health of the placenta and baby. Women with complications like diabetes, high blood pressure and an elevated BMI (body mass index), among others, are therefore generally advised to induce labour before the 40-week mark.
“This study explored some of these high-risk pregnancies to better understand what occurs or changes in the placenta with the goal of eventually developing better tests,” says Dr. Barbra de Vrijer, High-Risk Obstetrician and Head of Maternal Fetal Medicine at London Health Sciences Centre and Scientist at Lawson.
The St. Joseph’s Health Care London Perinatal Database, containing information on nearly 70,000 births between 1990 and 2011, provided the data for the study, including birth weight, placental weight and umbilical cord oxygen levels.
The study found that the number of blood vessels in the placenta (called vascularity) likely impacts oxygen in the umbilical vein, causing a slight increase in mothers with gestational diabetes, but a decrease in those with pre-existing diabetes.
Surprisingly, this new research indicates that hyper-vascularity in diabetic placentas (too many blood vessels) may actually decrease oxygen transfer, potentially leading to more risk to the baby.
“When there is an increase in placental vascularity, crowding of the blood vessels can occur constraining their effective absorbing surface area for oxygen uptake from maternal blood within the placenta,” says Dr. Bryan Richardson, Scientist at Lawson.
Another finding of the study confirmed earlier research showing that in women with both pre-existing and gestational diabetes, who tend to have larger babies, the placentas were also disproportionately larger, which is an indicator of decreasing placental efficiency, or the birth to placental weight ratio.
While additional research is needed, Dr. de Vrijer sees hope in the development of newer tests that look at factors like metabolic markers – the results of which could help indicate if the placenta is insufficient and assist in decisions like whether and when to induce labour.
“There are new technologies that we are looking at studying moving forward,” says Dr. de Vrijer. “Our team is focused on continuing our research to better understand high-risk pregnancies with a goal of continuously improving care for pregnant individuals.”
Standing up to falls
By merging world class care with research and artificial intelligence, St. Joseph’s Health Care London is catching falls before they happen.
They wreak havoc on independence and well-being, making them one Canada’s most pressing health challenges: falls.
A leading cause of injury-related hospitalizations, even death, among older adults, a fall can happen anytime, anywhere – with 50 per cent occurring at home. But what if we could predict and prevent falls before they happen?
A pioneering initiative at St. Joseph’s Health Care London (St. Joseph’s) is doing just that. The 3FM Clinic, short for Falls, Fractures, Frailty and Mobility, at St. Joseph’s Parkwood Insitute is at the leading edge of falls prevention in Canada, integrating research with clinical practice to offer hope and practical solutions to older adults.

Led by St. Joseph’s geriatrician Dr. Jaspreet Bhangu and Western University rehabilitation scientist and physiotherapist Janelle Unger, PhD, the visionary 3FM Clinic is working to prevent falls before they happen.
“We know there are a number of factors that can cause an older adult to fall such as illness, medication side effects, balance and gait issues, cognitive impairment, visual changes and environmental hazards,” says Bhangu. “What we’re working to understand is how those factors together impact individual patients and their risk of falling.”

To do so, the 3FM Clinic team – one of the largest, most diverse teams of its kind in the country – completes a multi-step evaluation of patients:
- Nurses gather their medical history, current medications, functional abilities and personal goals.
- Physical therapists measure the patient’s gait (how they walk) and balance to understand their physical capabilities.
- Occupational therapists test their vision, cognitive function and identify issues that might hinder the individual’s ability to perform routine tasks safely.
- A geriatrician focuses on medical risk factors such as bone health, medications and cardiovascular health to help manage risks associated with aging. The team then creates a customized care plan that incorporates exercises, therapeutic interventions and educational strategies.
On the research side, Unger and her team in the RED Neuro Lab at St. Joseph’s Gray Centre for Mobility and Activity are leveraging artificial intelligence (AI) to predict falls more accurately.
“Traditional fall prediction models often rely on limited data and lack real-world input from clinicians and patients,” explains Unger. “By partnering with Bhangu and the clinical team, as well as the patients in the 3FM Clinic, we’re able to integrate clinical information with biomechanical data collected from wearable sensors known as inertial measurement units (IMUs).”
An IMU is a device that tracks and measures a person’s movement and orientation and provides valuable data on how that person moves and stays stable.
“We plan to use AI to analyze the data collected through the IMU’s and are working to create accurate fall prediction models,” says Unger. “This research, funded by Western’s Bone and Joint Institute, has the potential to improve care decisions, enhance preventive strategies and ultimately reduce the incidence of fall-related injuries and hospitalizations for our patients and people across the globe.”
By embracing innovative research and compassionate care, the 3FM Clinic is a model for future efforts in fall prevention and geriatric care, offering a safer, more independent future for older adults.
You can prevent falls too:
- Use assistive devices: Properly fitted walkers or canes provide essential support and stability.
- Fitted footwear: Shoes (not slippers or flip-flops) with appropriate tread and low heels help prevent slips and falls. They should also fit your feet.
- Home improvements: Improved lighting, clear walkways and assistive bathroom fixtures.
- Exercise: Participate in strength and balance exercises to enhance physical fitness.
- Medication reviews: Regularly have your medications reviewed to identify if you are at risk of falling.
Study offers hope for hard-to-treat type 2 diabetes
A landmark international study involving patients and researchers at St. Joseph’s Health Care London shows automated insulin pump delivery can be ‘life-changing’ for people with type 2 diabetes

Lisa Mercer had tried just about everything to regulate the ups and downs of her blood sugars, from a strict diet to medication to four-a-day-day insulin shots.
But her busy life with type 2 diabetes finally started to feel better when she enrolled in a clinical trial at St. Joseph’s Health Care London to test the effectiveness of a system that combined glucose monitoring with an automated insulin pump.
“It was life-changing for me. I was diagnosed with type 2 diabetes 25 years ago and my blood sugars have always been all over the map. I felt sort of helpless. I said yes to this clinical trial because I hoped it would return some normalcy to my life,” she says. Now that study, with results newly published in the prestigious New England Journal of Medicine, is being heralded as a big step forward for patients with hard-to-treat type 2 diabetes.
“This is an exciting finding because it shows we can improve patients’ blood sugars and hopefully prevent long-term negative consequences of high sugars while at the same time making it easier for patients to manage the disease,” says Dr. Tamara Spaic, Medical Director of St. Joseph’s Diabetes Education Centre and the lead Canadian researcher for the multi-site international study based at the Jaeb Center for Health Research in Tampa, Fla.
Study participants were placed either in a group testing the effectiveness of a new system called Control IQ+ or a control group continuing their existing diabetes management regimen.

The intervention group wore glucose monitors that electronically talked with high-tech pumps that delivered insulin – automatically, in the right dose and at the right time – with minimal patient input.
While the device was approved about five years ago for people with type 1 diabetes, this is the first examination of its effectiveness managing the complexities of type 2 diabetes.
“The biggest burden in diabetes control is that it’s 24/7 vigilance: did I eat or not; what did I eat and how much; did I exercise; do I need to wake up for an insulin shot in the middle of the night? This system largely removes those variables to bring blood sugars to target levels,” says Spaic, who is also a Lawson Research Institute scientist and professor of endocrinology and metabolism at Western University’s Schulich School of Medicine & Dentistry.
“What surprised us was that this worked so well across all populations regardless of duration of the disease, amount of insulin needed, whether they used other medications or not, whether they were tech-savvy or not. It worked for everyone regardless of their ethnicity, socioeconomics, and whether they were male or female, old or young,” she adds.
Researchers even asked participants in the intervention group to skip insulin with meals on occasion – generally a no-no in the highly regimented life of someone with insulin-managed diabetes – and the automated system responded appropriately and quickly to adjust blood sugars.
Mercer found improvement within a couple of weeks: “Before the pump, I felt awful. When my sugars were too low, I got the shakes, I had trouble communicating and thinking clearly and I got extremely tired. When my sugars were too high, I was exhausted. It dominated every day and was tough on my job as a police officer. Now I feel better. I feel more in control.
“Is it perfect? No. But my sugars are stable and consistent more often than not.”
Not yet approved in Canada

In February, the US Food and Drug Administration cleared the use of the Control IQ+ system in adults with type 2 diabetes – approval that also meant the expense could be covered through health insurance.
However, it has not yet been brought to Health Canada regulators for approval, Spaic says.
Even so, several of her patients, including Foster, decided to continue using the system after the 13-week trial, paying out-of-pocket or through private insurance.
Spaic and St. Joseph’s colleagues, endocrinologist Dr. Selina Liu and nurse coordinator Marsha Driscoll, were extensively involved in the design of the study, recruiting and monitoring participants and reporting results.
Diabetes type 2 usually develops in adulthood and is a condition in which body cannot make enough insulin or does not properly use the insulin it makes to regulate the amount of glucose (sugar) in the blood.
While most people with type 2 diabetes can control their blood sugars through lifestyle changes or with new treatments such as non-insulin glucose-lowering medications, the sub-set of North Americans who require insulin still numbers in the millions.
THE STUDY:
What: 13-week, large-scale clinical trial to test the effectiveness of a system combining automated insulin delivery with continuous glucose monitoring for people with type 2 diabetes.
Who: 319 study participants – including 13 at Lawson Research Institute of St. Joseph’s Health Care London – all needing multiple daily insulin doses. Age range 19 to 87, from 21 centres across the U.S. and Canada. Study led by Jaeb Centre for Health Research in Tampa, Fla., and funded by Tandem Diabetes Care, which also provided the automated insulin-delivery systems
How: Two-thirds of patients received an automated insulin pump, continuous glucose monitor and transmitter to track and automatically administer insulin to regulate their blood sugars. A control group continued their existing insulin-delivery method and also received glucose monitors.
Results: The intervention group had more stable blood sugar levels – with 3.4 more hours per day in the target glucose range – than the control group. Use of automated insulin devices was successful and safe even for patients without previous experience with an insulin pump
Why it matters: Automated insulin delivery can help insulin-dependent patients manage their type 2 diabetes better than before. Better management means improved quality of life and may result in fewer diabetes complications such as heart disease and damage to the eyes, kidneys and nerves.
Why healthy aging means caring for both brain and body
This story was first published nationally by the Canadian Institutes of Health Research to spotlight health-research stories with impact.
Judith and Matthew are among eight million people in Canada aged 65 years and older. Lately, both noticed changes in how they moved and how well they remembered things. So they went to see their doctor.

Their experiences took different turns. Judith was referred to a physiotherapist, but her memory problems went unnoticed. Matthew was sent to a memory clinic, yet no one asked him if he had fallen recently or was having difficulty walking.
This type of fragmented care is exactly what Dr. Manuel Montero-Odasso, a geriatrician and researcher at Lawson Research Institute (Lawson) of St. Joseph’s Health Care London, has been trying to change for decades. His research shows that brain health and mobility are deeply connected throughout the aging process.
“As we get older, our mobility and cognition may decline, which can be worsened by mild cognitive impairment and dementia,” explains Montero-Odasso. “But that doesn’t have to be our destiny.”
To improve the physical and brain health of older adults, Montero-Odasso advocates for a more holistic approach to care –one that addresses the full spectrum of aging challenges, from dementia to decline in mobility, from Alzheimer’s to the risk of falls. His CIHR-funded research on these topics has been supported by the Canadian Consortium on Neurodegeneration in Aging.

One of his projects led to a national consensus that recommended 10 mobility and cognitive tests that assess a range of functions—from walking speed to the ability to walk and talk at the same time. These recommendations have helped make the diagnosis of physical and cognitive impairments in older adults more consistent and standardized.
Under Montero-Odasso’s leadership, the Mobility, Exercises and Cognition team has looked at how physical and cognitive training together can improve health in older adults. Findings from two major studies, the SYNERGIC Trial and Synergic at Home Trial, showed that combining aerobic and resistance exercises (such as using bands and weights) with cognitive challenges is particularly effective. The team designed a personalized program that keeps the brain fit, from memory to executive function.
This combined approach not only slows cognitive decline but also improves mobility and brain health. Even more encouraging, the benefits lasted for up to a year. The team also found that not all physical activities are equal when it comes to protecting cognition.
“Walking is great for your cardiovascular health, but not enough to prevent or delay dementia. We need a mix of aerobic and resistance exercises combined with cognitive training,” says Montero-Odasso.

Building on these findings, the Mobility, Exercises and Cognition team is developing clinical guidelines to help health professionals prescribe lifestyle-based activities such as physical and cognitive training to treat mild cognitive impairment, a condition that can lead to dementia.
Dr. Montero-Odasso’s holistic approach to older adult care also focuses on preventing falls, a major issue affecting one-third of seniors worldwide. After identifying significant gaps in clinical practice around the globe, he and experts from 40 countries developed the World Fall Prevention Guidelines.
Endorsed by the Canadian Geriatrics Society and adopted in countries including Australia, Belgium, China, Malaysia, and Norway, the guidelines are the first to incorporate the patient perspective and to consider key factors such as cognition, walking speed, balance, and even fear of falls. These guidelines provide practical tools such as an algorithm that predicts the risk of falls and recommends targeted interventions.
When asked why focusing on both brain and body should be a priority for Judith, Matthew, and the other 18% of Canadians over 65, Dr. Montero-Odasso shares a powerful message: “We don't stop moving and develop mobility disability because we age. We age because we stop moving. But it’s never too late to make some lifestyle changes.”