Search
Search
159 Search Results:
… 2 Our People … care, recovery, discovery, teaching and resiliency – of our teams, our patients and residents, and their families. … a magistral demonstration of the beauty and art of the… management of renal and ureteral stones. We are deeply … In a unique project, she is creating a series of 12 oil paintings on canvass depicting various aspects of radiology …
Annual Report 2016-2017 Welcome to the 2016-2017 Annual Report Contents Annual Report 2016-2017 .......................................................................................................... 1 Welcome to the 2016-2017 Annual Report ...........................................................
… 4 Commitment to our patients … CEO; and Roy Butler, Vice President Patient Care and Risk Management. Back row from left are: Dr. Charles Nelson, … of creative experiences to choose from, including drawing, painting, print making and textile art. • Storytelling and …
Annual Report 2017-2018 Welcome to the 2017-2018 Annual Report Contents Annual Report 2017-2018 .......................................................................................................... 1 Welcome to the 2017-2018 Annual Report ...........................................................
… tremendous accomplishment - a testament to the tenacity of our staff, physicians and volunteers and their unwavering … therapy (CBT) program that combines mindfulness-based pain management and practical life applications guided by a … therapy (CBT) program that combines mindfulness-based pain management and practical life applications guided by a …
Moving forward together St. Joseph's Report to the Community 2021-2022 An unrelenting pandemic has meant another historic year for St. Joseph's Health Care London. Yet it has also been a year of tremendous accomplishment - a testament to the tenacity of our staff, physicians and volunteers and their...
… and research. sjhc.london.on.ca V_01Jan212021 How to join your education session Marilyn Hill, C. Psych. i,.. SI … JOSEPHs HEALTH CARE LONDON Table of Contents How to join your education session … How to join your education session … Before your session: … 24 How Your Heart Works …
t~ STJOSEPHs HEALTH CARE LONDON Cardiac Rehabilitation and Secondary Prevention Program Patient Education Guide CARING FOR THE BODY, MIND & SPIRIT SINCE 1869 Renowned for compassionate care, St. Josephs is one of the best academic health care organizations in Canada ...
… cancer outcomes. For St. Joseph’s, it is the generosity of our donors that makes these possibilities a reality. In … in their lifetime, a condition that causes excruciating pain often compared to childbirth. The lithotripter, a … Hospital, a new clinical research centre will address the management of complex chronic diseases such as diabetes, …
Community Stewardship Report 2014 2015 An average day at St. Josephs is filled with possibilities, whether its through innovative approaches to treatment or the potential offered by new medical technologies. Each day, these seemingly endless possibilities can be measured in the way people recovering...
… possible. Just one of the reasons why YOU HELPED ENHANCE OUR OPERATING ROOMS 2019–2020 Community Impact Report Your … symptoms related to their traumatic injury or chronic pain to iCBT. In The MacDonald/Franklin Operational Stress … on the health and well-being of people in our region. MANAGEMENT/STEWARDSHIP The financial performance of the past …
Back row left: Holly Bridge, Diane Davis-Miller, Barb Simmonds Front row left: Dr. Jennifer Bjazevic, Roger Blum, Leanne Summers, Dr. Hassan Razvi, Surgical Services You make health care innovation possible. Just one of the reasons why YOU HELPED ENHANCE OUR OPERATING ROOMS 20192020 Community Impact...
… the difference on pg. 3. 2020–2021 Community Impact Report Your donation matters here. THANK YOU FOR HELPING US RESPOND … five major spinal surgeries, Phil was left with constant pain and no clear direction on next steps for his physical … The online therapy— which combines mindfulness-based pain management and practical life applications guided by a …
In response to COVID-19, care providers across St. Josephs quickly and expertly pivoted to meet challenges during the pandemic. Seen here, team members from the Urgent Care Centre at St. Josephs Hospital. Learn how donors made all the difference on pg. 3. 20202021 Community Impact Report Your donati...
… decisions about end-of-life care long before the Supreme Court of Canada decision and medical assistance in dying … or her physical and emotional condition such as excessive pain, suffering, expense or other serious inconvenience, as … to best practices in palliative care, chronic disease management (including chronic pain) and suicide prevention. …
End-of-Life Care Contact St. Josephs Health Care London St. Josephs supports individuals making informed decisions about their end-of-life care. This includes talking with family, planning ahead when possible, and deciding when to decline or withdraw treatment (to allow natural death). Patients and ...
… Health Care, London is required to prepare and make public our Year Four accessibility plan and report on Year Three … & Public Affairs Phyllis Brady Patient Relations / Risk Management Beth Schroeder Volunteer Services / Patient … in providing services to persons affected by chronic pain. Attitudinal Increase awareness of Sign language …
Annual Accessibility Plan for St. Josephs Health Care, London September 2007 - August 2008 Submitted to Cliff Nordal Chief Executive Officer 30 September 2007 Prepared by SJHC Accessibility Working Group Co-ordinator, Derek Lall This publication is available on the St. Josephs Heath Care, Londons we...
… Health Care, London is required to prepare and make public our Year Seven accessibility plan and report on Year Six … & Public Affairs Phyllis Brady Patient Relations / Risk Management Terry Kaban Ivey Eye Institute Susan Vuylsteke … in providing services to persons affected by chronic pain. Attitudinal Increase awareness of Sign language …
Annual Accessibility Plan for St. Josephs Health Care, London September 2008 - August 2009 Submitted to Cliff Nordal Chief Executive Officer 30 September 2008 Prepared by SJHC Accessibility Working Group Chair, Derek Lall This publication is available on the St. Josephs Heath Care, Londons website a...
… a parent or legal guardian is required. • A maximum of four essential caregivers may be designated per resident at a … access to the support of their family as part of the care team. Essential caregivers typically support activities of … or taste disorder(s) • Nausea/vomiting, diarrhea, abdominal pain • Runny nose or nasal congestion (in the absence of an …
HEALTH CARE LONDON ESSENTIAL CAREGIVER COVID-19 GUIDELINES AND EDUCATION REQUIREMENTS ~~ STJOSEPHs HEALTH CARE LONDON Essential Caregiver COVID-19 Guidelines and Education Requirements Caregiver A caregiver is defined in the Fixing Long-Term Care Act, 2021, O. Reg 246/22 section (4) as follows: a. i...
… Care Parkwood Institute Teams, clinics and programs in our community and beyond ST. JOSEPH’S IS PAGE 2 OF 4 St. … Disease Program • Otolaryngology – Head & Neck Surgery • Pain Management Program • Peripheral Nerve Clinic • Regional … Disease Program • Otolaryngology – Head & Neck Surgery • Pain Management Program • Peripheral Nerve Clinic • Regional …
Care Matters Here. Learn More. sjhc.london.on.ca BODY | MIND | SPIRIT Leena Justus Registered Nurse Mount Hope Centre for Long Term Care Renowned for compassionate care, St. Josephs is one of the best academic health care organizations in Canada, dedicated to helping people live their fullest by mi...
… care, earning the complete confidence of those we serve. Your care matters here. Renowned for compassionate care, St. … Disease Program • Otolaryngology – Head & Neck Surgery • Pain Management Program • Peripheral Nerve Clinic • Regional … Disease Program • Otolaryngology – Head & Neck Surgery • Pain Management Program • Peripheral Nerve Clinic • Regional …
Leena Justus Registered Nurse Mount Hope Centre for Long Term Care St. Josephs provides exceptional care, earning the complete confidence of those we serve. Your care matters here. Renowned for compassionate care, St. Josephs is one of the best academic health care organizations in Canada, dedicated...
First clinical guidelines in Canada for pain following spinal cord injury
Researchers at Lawson Health Research Institute are the first in Canada to develop clinical practice guidelines for managing neuropathic pain with patients who have experienced a spinal cord injury (SCI).
Neuropathic pain is complex and chronic, and is the most common complication reported by people following SCI. The research team worked with care providers at Parkwood Institute, part of the St. Joseph’s Health Care London family, and an international panel to address the complex and unique challenges for managing pain during recovery and rehabilitation.
In 2003, Dan Harvey sustained a spinal injury after falling off a trampoline. Using his personal experience, as well as his experiences meeting with newly injured people, Harvey contributed to the development of the new guidelines.
“Neuropathic pain – and pain in general – affects every person with a spinal cord injury very differently. Some people have it, some people don’t. But for those who do have it, it can make rehabilitation and recovery much more difficult,” explains Harvey.
“On top of just learning how to use your body again, you also have to deal with various forms of physical pains, which can make it challenging to mentally adapt to an injury.”
For those with chronic pain, it may be hard to just get out of bed in the morning, feel well enough to leave the house, or even fall asleep. “I have fairly extensive neuropathic pain, so I’m well aware of how difficult it can be to get a full night’s sleep, or show attentiveness at work or at school when it literally feels like your legs are on fire,” says Harvey.
Image

Dan Harvey with Lawson researchers Stacey Guy, Swati Mehta and Dr. Eldon Loh.
Dr. Eldon Loh, Lawson Researcher and Physical Medicine and Rehabilitation Specialist at St. Joseph’s, and his team recognized that pain can be an overlooked part of a spinal cord injury and plays a major factor in the success of rehabilitation. It’s difficult for someone in pain to participate fully in their own recovery, and so long-term disability becomes more likely. Pain is difficult to manage and it often takes multiple approaches to find something that works for each person.
“This is a starting point for us to standardize how we approach pain in the clinic. We have identified gaps and offered recommendations to not only manage the pain, but also ensure that our patients can fully benefit from rehabilitation,” says Dr. Loh.
The results of the three-year process led to recommendations for screening and diagnosis, treatment and models of care. Important clinical considerations accompany each recommendation.
“For those in hospital following an injury, it’s about making sure they can be as independent as possible before discharge. Over time, we want to keep pain levels under control so that they are able to live life to the fullest,” adds Dr. Loh.
The research will inform new tools and resources for care providers and patients.
Harvey believes the guidelines will have a tremendous impact for patients whose pain may have been overlooked. “Pain can be created through many different avenues and the effects can snowball after a person is discharged and sent home. If you don’t check all of the boxes, you might be missing a very important item.”
The new guidelines have been published in the international journal Spinal Cord. The Ontario Neurotrauma Foundation and Rick Hansen Institute provided funding for the research study.
A special thanks to individuals from St. Joseph's who were involved in the project: Steve Orenczuk, Patrick Potter, Keith Sequiera, Lindsey Guilbault, Robert Teasell, Anna Kras-Dupuis, Dalton Wolfe, Alba Casalino and Dwight Moulin.
Image

Additional members of the panel that developed the new clinical practice guidelines.
… tissue injury, musculoskeletal injuries and generalized pain. iPod Project - Music and Memories, $4,803 - Mount Hope … with families and friends in a camp-like setting, which encourages socialization, building new skills and kindling fond … Program, Parkwood Institute, Main Building One-hundred self-management resource kits were created to be used as a tool …
1 | P a g e 2015/16 LIST OF GRANTS PAID Patient Care Grants Hydrocollator, $2,955 - Mount Hope Centre for Long Term Care Physiotherapists will use a hydrocollator to provide therapeutic heat that will help to treat residents for various conditions, including arthritis, soft tissue injury, musculoske...
… Health Care Foundation – 2016/17 Allocations The Endourology Fellowship Program, $25,000 - St. Joseph's Hospital … day of outdoor carnival type activities, along with face painting, treats and a live band. Patient Satisfaction … minute details and produces 3D images, Dr. Dhanvantari’s team is currently the only research group in the world …
St. Josephs Health Care Foundation 2016-17 Allocations MEDICAL COLLABORATION London Medical Innovation and Commercialization Network City Innovation Grant, $4,013,287 PATIENT CARE Chapel Refurbishment, $195,000 - St. Joseph's Hospital The 100-year-old chapel at St. Josephs Hospital received upgrades...
… a home-like atmosphere where people at the end of life’s journey can live, and die, with dignity. Zero Suicide, … day of outdoor carnival type activities, along with face painting, treats and a live band. Canada 150 Mount Hope Art … Health Care Awarded to members of an interdisciplinary team providing or supporting clinical care, four awards were …
St. Josephs Health Care Foundation 2017-18 Allocations PATIENT CARE Life Experiences in Complex Care, $3,049 Parkwood Institute Main Building Patients in the Complex Care Program were able to attend various community outings, while those who were unable to leave were provided with special on-site p...
Growing Tissues in the Lab
When challenged by surgeons to find better treatments for difficult-to-manage connective tissue diseases, Dr. David O’Gorman gladly accepted.
Dr. O’Gorman is a Molecular Biologist and Lawson Scientist based at St. Joseph’s Hospital, a part of St. Joseph’s Health Care London. His research focuses on understanding normal and abnormal connective tissue repair. He collaborates with researchers and clinicians working in many different disciplines, including those specializing in reconstructive surgery, orthopedics and urology.
Surgical reconstructions can be hampered by a lack of graft tissue, or graft tissue of insufficient quality, making it difficult to achieve optimal outcomes for the patients.
An example is a condition called urethral stricture disease (urethral scarring). This condition occurs in males and typically causes symptoms such as frequent and urgent urination, and slow urinary stream. In extreme cases, it can cause urinary tract infections, permanent bladder dysfunction and renal failure. Recurrence rates after minimally invasive treatments are high, and so many urologists recommend open surgical approaches.
Surgeons can use the patient’s own tissues to reconstruct the urethra after stricture removal. This tissue is normally sourced from the buccal cavity in the mouth but taking large tissue grafts can result in complications. In cases where buccal grafts have been used for previous reconstructions, there may not be enough intact tissue left.
Dr. O’Gorman sees a solution in growing sheets of human buccal tissues in the lab.

“We are currently using buccal graft trimmings as a source of cells, culturing them in a 3D environment and expanding them to create tissues of suitable size, density and elasticity.”
The patient’s own cells are used to generate a tissue graft for urethral reconstruction. While several research groups have developed this approach in the past, few have attempted to translate their models for clinical use.
“Our immediate goal is to provide proof of principle – that we can consistently generate grafts of suitable size and functional characteristics,” explains Dr. O’Gorman, “In the future, we could be providing bioengineered graft tissues for reconstructive surgeries here in London.”
Bioengineered human tissues can also be used as ‘mimetics’ – replications of human tissues – to study diseases, especially those difficult to model using routine laboratory methods.
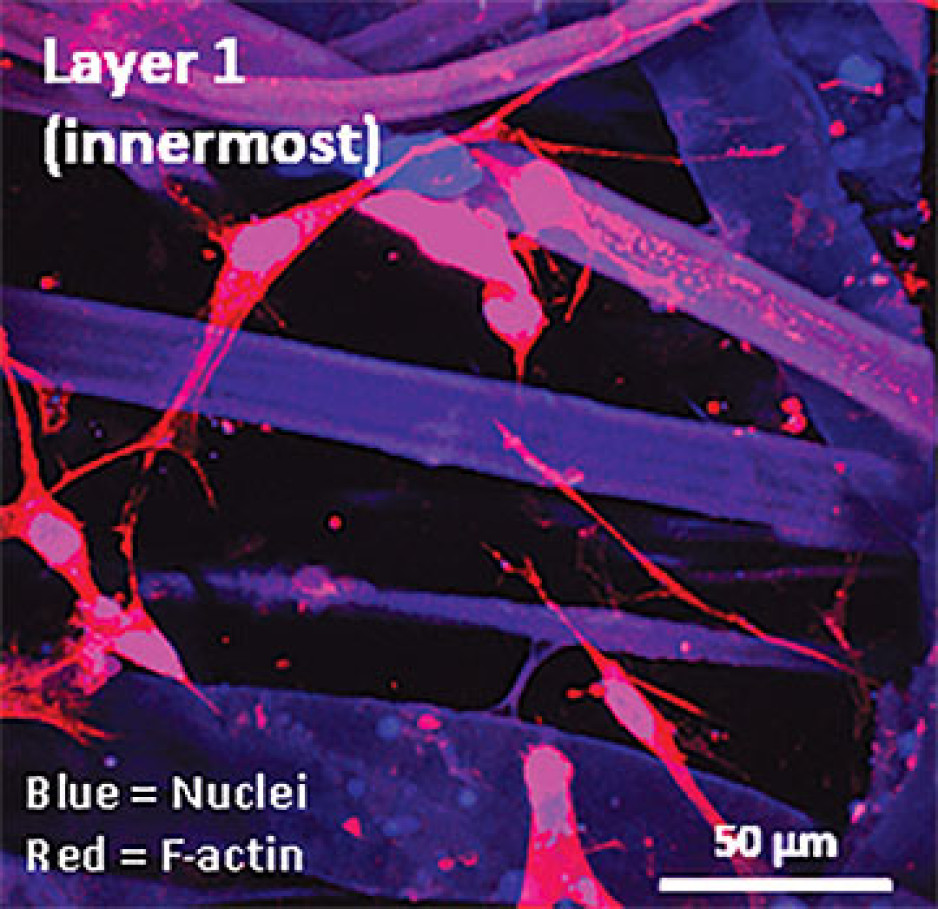
Instead of a using a growth media or sterile plastic dishes, 3D cell culture is achieved by embedding cells in a matrix of proteins and other molecules normally found in those tissues. In this environment, gene expression and growth is more similar to cells of connective tissues in the body being replicated.
Dupuytren’s disease (or Dupuytren’s Contracture) affects the palmar fascia in the hand, a connective tissue beneath the skin that extends from the base of the palm into the fingers. This disease can be understood as a type of excessive scarring, where normal tissue repair processes have gone awry and dense scar tissue forms, typically causing permanent palm or finger flexion that restricts hand function.
This condition is surprisingly common and may affect more than one million people in Canada. While there are surgical treatment options available, none consistently prevent this disease from recurring in at least a third of patients.
“Due to its high recurrence rate after treatment, Dupuytren’s disease is currently considered incurable. Our challenge is to understand it well enough to develop truly effective treatments,” says Dr. O’Gorman.
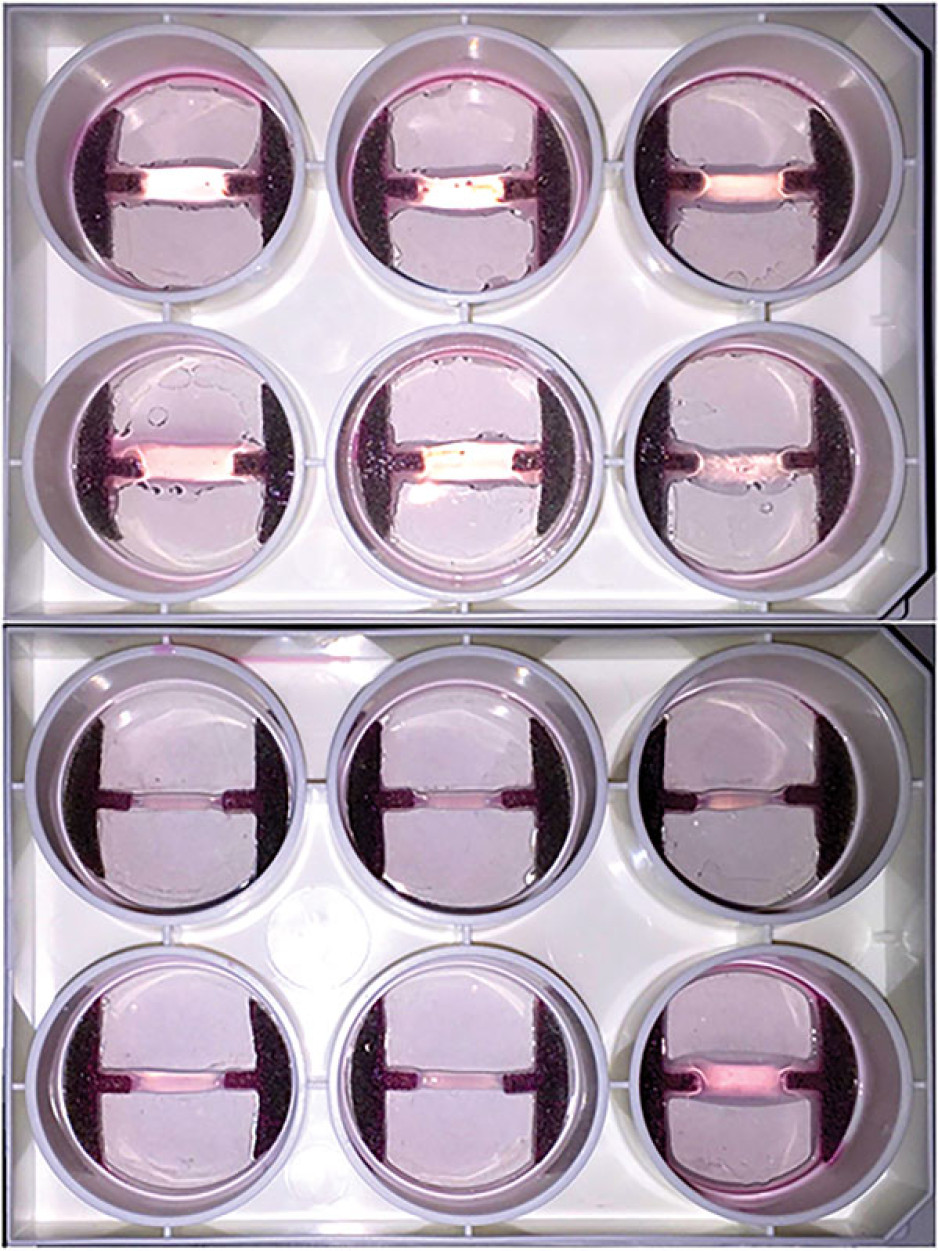
Human hands have unique characteristics not found in other species, making animal models impractical. Instead, Dr. O’Gorman’s team extracts cells from the diseased palmar fascia of patients undergoing hand surgeries and bioengineers them into palmar fascia ‘contractures’ in the lab.
“Since the cells from a single palmar fascia sample can be used to grow dozens of little contractures, we can test many different treatments simultaneously to see what works best for each patient.”
This approach may also allow them to determine if Dupuytren’s disease is truly one disease, or a group of similar diseases that cause palm and finger contractures.
“Often, Dupuytren’s disease is clearly heritable, but some individuals have no family history of it and develop apparently sporadic disease,” notes Dr. O’Gorman. “We want to determine if these are truly the same disease at the molecular level.”
Another major cause of abnormal connective tissue repair is infection, and tissue mimetics can play a role here, too. While rare, infections of artificial joint replacements are particularly devastating for patients, as they typically require readmission to hospital to remove the infected joint, weeks of antibiotic-based treatment, and an additional surgery to replace the artificial joint.
In addition to the associated pain and suffering, these procedures are technically challenging and costly to our health care system.

Artificial shoulder joint infections are most frequently caused by the microorganism Cutibacterium acnes (C. acnes). C. acnes infections disrupt normal tissue repair processes after surgery, cause shoulder tissues to die and promote loosening of the artificial joint. These infections are difficult to diagnose, and there is a lack of reproducible
models in which to study them. Dr O’Gorman’s team has set out to create the first human Shoulder-Joint Implant Mimetic (S-JIM) of C. acnes infection.
“While S-JIMs are more complex, they are 3D in vitro cell culture systems designed to mimic human tissues, like those that we use for studying Dupuytren’s disease.”
S-JIMs include layers of artificial human tissue, wrapped around cores of titanium alloy or cobalt chrome, the metals used to create artificial joints. They are co-cultured with C. acnes under low oxygen conditions similar to those that normally occur around artificial shoulder joints.
“We are bioengineering simple 3D cell cultures to more closely mimic the complexity of human tissues, with blood supply, nerves and interactions with other cells.” – Dr. David O’Gorman
Studying the connective tissue layers close to the infection allows researchers to investigate processes that promote infection, such as the formation of a biofilm that harbours and protects the bacteria from the body’s immune system. They are also able to test whether novel treatments can disrupt biofilm formation and increase the effectiveness of antibiotics.
Dr. O’Gorman predicts that in the future, medical researchers will routinely use bioengineered 3D human tissue and organ mimetics to accelerate our understanding of disease.
“The technology is in its infancy, but the potential for using bioengineered human tissues for surgical reconstructions or as disease models is huge. At Lawson, we’re ready to take on health care challenges and build on innovative approaches to improve the quality of life for patients.”
ONLINE EXCLUSIVE: What is 3D cell culture?
Medical researchers have grown human cells in culture media on or in sterile plastic dishes, such as Petri dishes, for more than 50 years.
Some cells, such as blood cells, can survive and grow in suspension, while others like smooth muscle cells need¬ to adhere to a surface to survive and grow. These are often called “2D cell cultures” because the cells grow horizontally across the bottom of the dish.
Some cells derived from connective tissues, such as fibroblasts, are not only adherent, but also very sensitive to the stiffness of their environment (“biomechanically sensitive” cells). Plastic dishes are at least 10,000 times stiffer than most connective tissues, and when biomechanically sensitive cells detect stiff surfaces, they can change the expression of their genes and behave abnormally.
The most common proteins in these tissues - and in the entire human body - are collagens, and one routine 3D cell culture approach is to embed fibroblasts in a collagen gel (gelatin). Fibroblasts in this environment can grow in any direction they choose, and their gene expression is more similar to cells in connective tissues.
These simple 3D cell cultures represent tissue engineering in its most basic form.
“Our challenge is to bioengineer simple 3D cell cultures in the lab to more closely mimic the complexity of human tissues, which have blood supply, nerves and interactions with other cells and tissues that modify their function and ability to heal after injury,” explains Dr. O’Gorman.
Dr. David O’Gorman is a Lawson Scientist and Co-director, Cell and Molecular Biology Laboratory at The Roth | McFarlane Hand and Upper Limb Centre in London, Ontario. He is also an Assistant Professor at Western University.
… Resource Guide to Insulin Pump Success Acknowledgements The team at the Diabetes Education Centre of St. Joseph’s Health … 4.5 Sick Day Management … Thirst Excessive urination Fatigue Abdominal pain, nausea, vomiting Blurred vision Change in appetite …
Resource Guide to Insulin Pump Success Acknowledgements The team at the Diabetes Education Centre of St. Josephs Health Care London would like to thank Sanofi-Aventis for their generous contribution to sponsoring this educational initiative, thereby encouraging further development of resources and d...
… 19 PERFORMANCE MANAGEMENT AND IMPROVEMENT … them good care when they are sick and will be there for our children and grandchildren". Roles, I .2.1 ' MOHLTC's … Cardiac Conditions Arrhythmia Angina Pectoris Chest Pain Other GI Diagnoses Cirrhosis and Alcoholic Hepatitis …
SOUTH WEST LOCAL HEALTH INTEGRATION NETWORK (the LHIN) and St. Josephs Health Care, London (the H os p i ta I) Hospital Service Accountability Agreement for 2008-1 0 HospitaI Service Accountability Agreement for 2008-1 0 TABLE OF CONTENTS l a O BACKGROUND ..............................................