Search
Search
898 Search Results:
… must be notified to ensure consistent, organized action planning. • ENS 2 is immediately activated for Code Green, … The 11\IS Structure ----- Operations Section "Doers" Scribe Planning Section "Thinkers" Liaison Logistics Section … role (incident manager) with operations (the doers), planning (the thinkers), logistics (the getters) and …
(yj~ SIJOSEPHs HEALTH CARE LONDON Evacuation Fire Hazardous Chemical Spill Bomb Threat/Suspicious Object Critical Infrastructure Failure External Disaster YELLOW Missing Person WHITE Violent Person Hostage Taking Person with a Weapon Adult Medical Emergency Pediatric Medical Emergency Emergency Colo...
~~ STJOSEPHs HEALTH CARE LONDON Emergency Management Committee Terms of Reference Purpose: The Emergency Management Committee is responsible for supporting an effective organization-wide emergency management program. Key Functions: Review the organizations emergency response procedures and Emergenc...
… their end-of-life care. This includes talking with family, planning ahead when possible, and deciding when to decline … their end-of-life care. This includes talking with family, planning ahead when possible, and deciding when to decline …
End-of-Life Care Contact St. Josephs Health Care London St. Josephs supports individuals making informed decisions about their end-of-life care. This includes talking with family, planning ahead when possible, and deciding when to decline or withdraw treatment (to allow natural death). Patients and ...
… management plan will be presented to our corporate Resource Planning Council to allow for further education and … management plan will be presented to our corporate Resource Planning Council to allow for further education and …
Energy Conservation and Demand Management Plan Made for Ontario Regulation 397/11 Green Energy Act, 2009 Authored by: Mark Read June 18, 2014 2 The Green Energy Act - Regulation 397 The Energy Conservation and Demand Management Plan outlined in the following report is the second component of a two p...
… Group 6 5. SJHC’s, London commitment to accessibility planning 6 6. Recent barrier-removal initiatives 7 7. … Steering Group. Derek Lall, Co-ordinator, Facilities Planning and Development, is the Chair of SJHC Accessibility Working Group. Karen Trower, Facilities Planning and Development is the Co-chair of SJHC …
Annual Accessibility Plan for St. Josephs Health Care, London September 2008 - August 2009 Submitted to Cliff Nordal Chief Executive Officer 30 September 2008 Prepared by SJHC Accessibility Working Group Chair, Derek Lall This publication is available on the St. Josephs Heath Care, Londons website a...
… plan has been changed to align with St. Joseph’s business planning cycle. The time period for this plan runs from … 4. Planning cycle … in appendix 1. Roy Butler, Integrated Senior Director of Planning and Operational Improvement, is the senior leader … is chairing the Accessibility Working Group and leading the planning process. While some members of the working group …
Annual Accessibility Plan October 2009 March 31, 2011 Submitted to the St. Josephs Board of Directors, September 28, 2009 Prepared and Submitted by St. Josephs Accessibility Working Group St. Josephs Accessibility Plan September 28, 2009 2 Executive Summary St. Josephs Health Care, London, (St. Jos...
… Group 6 5. SJHC’s, London commitment to accessibility planning 6 6. Recent barrier-removal initiatives 7 7. … Steering Group. Derek Lall, Co-ordinator, Facilities Planning and Development, is the Co- ordinator of SJHC Accessibility Working Group. Karen Trower, Facilities Planning and Development is the Co-chair of SJHC …
Annual Accessibility Plan for St. Josephs Health Care, London September 2007 - August 2008 Submitted to Cliff Nordal Chief Executive Officer 30 September 2007 Prepared by SJHC Accessibility Working Group Co-ordinator, Derek Lall This publication is available on the St. Josephs Heath Care, Londons we...
… 2 Planning cycle … Page 3 Members of the Accessibility Advisory Committee 3. Planning Cycle An annual status report will be prepared for … list was reviewed by the relevant services (e.g. Facilities Planning) that would be accountable for addressing the … 2 Planning cycle …
Accessibility Plan January 2013 December 2015 Submitted to St. Josephs Senior Leadership Team on January 8, 2013 Prepared and Submitted by St. Josephs Accessibility Advisory Committee Table of Contents St. Josephs Mission Statement. ...... 1 Introduction.. .............................................
… Working Group 6 5. Hospital commitment to accessibility planning 7 6. Recent barrier-removal initiatives 7 7. … Group. Derek Lall, Senior Project Consultant, Facilities Planning and Development, is the Co-ordinator of the SJHC … Working Group Member Department Derek Lall Facilities Planning and Development Purvi Desai Facilities Management …
Annual Accessibility Plan for the St. Joseph Health Care, London September 2005 - August 2006 Submitted to Cliff Nordal Chief Executive Officer 30 September 2005 Prepared by SJHC Accessibility Working Group Co-ordinator, Derek Lall This publication is available on the hospitals website and in altern...
CARING FOR THE BODY, MIND & SPIRIT SINCE 1869 Renowned for compassionate care, St. Joseph's is one of the best academic health care organizations in Canada dedicated to helping people live to their fullest by minimizing the effects of injury, disease and disability through excellence in care, teachi...
HEALTH CARE LONDON ESSENTIAL CAREGIVER COVID-19 GUIDELINES AND EDUCATION REQUIREMENTS ~~ STJOSEPHs HEALTH CARE LONDON Essential Caregiver COVID-19 Guidelines and Education Requirements Caregiver A caregiver is defined in the Fixing Long-Term Care Act, 2021, O. Reg 246/22 section (4) as follows: a. i...
… in the right place, at the right time. Therefore, when planning, reviewing, and delivering services we need to ask … with special needs, such as the homebound. Therefore, when planning, reviewing, and delivering services, we need to ask … decisions that allow them to live at risk. Therefore, when planning, reviewing, and delivering services to them, we …
Living Longer, Living Well Highlights and Key Recommendations From the Report Submitted to the Minister of Health and Long-Term Care and the Minister Responsible for Seniors on recommendations to inform a Seniors Strategy for Ontario Dr. Samir K. Sinha, MD, DPhil, FRCPC Provincial Lead, Ontarios Sen...
… judgment. Exemplifies accountability and advocacy in the planning and delivery of care. Actively contributes to … judgment. Exemplifies accountability and advocacy in the planning and delivery of care. Actively contributes to …
ST. JOSEPHS HEALTH CARE EXCELLENCE IN NURSING AWARDS 2008 NOMINATION FORM Name of Nominee: ____________________________________________ Site: ____________________________________________ Department: ____________________________________________ Title of Award: Excellence in Direct Care __________ (Pa...
Expanded No Fixed Address strategy houses half of those in danger of homelessness
At a community symposium on health care and homelessness attended by over 250 Londoners, a research team from Lawson Health Research Institute announced the results of a nine-month, federally funded project tackling the issue of homelessness from within hospital walls.
The No Fixed Address (NFA) strategy reaches and supports patients during the crucial transitional period when they are being discharged from the hospital and re-integrated into the community. The approach was initially tested with strong success for mental health patients across the city and the second ‘version’ of the project was extended to medical units at London Health Sciences Centre’s University Hospital and Victoria Hospital.
Image

“Many of our patients with lived experience of homelessness were saying that their journey started with a hospital discharge,” explains Dr. Cheryl Forchuk, Assistant Scientific Director at Lawson and NFA project lead. “They were often experiencing major transitions in their lives and then experienced a hospital stay. Normally a relatively short visit, they aren’t able to gather the information and make a plan to be able to leave the hospital with somewhere to stay.”
Through partnerships between service providers and non-profit organizations, the NFA strategy helps prevent homelessness by providing timely and accessible supports to patients who would otherwise be discharged into homelessness. Staff from the Canadian Mental Health Association Middlesex, Salvation Army’s Housing Stability Bank, and Ontario Works in the City of London provided direct, on-site patient access to housing and income support databases
“Lawson’s No Fixed Address research project is the first evaluation anywhere of a strategy that aims to reduce the number of hospital patients being discharged into homelessness,” says Dr. Forchuk.
Over nine months, 74 people experiencing medical health issues accessed the NFA program. Of those, 54 per cent were also experiencing mental health challenges.
All of the study participants were in imminent danger of homelessness. Through the supports provided as part of this research study, half were able to arrange housing before being discharged.
“We were able to help a lot of people, with 50 per cent successfully securing housing,” shares Dr. Forchuk. “With the results and feedback we received, we learned a lot about how we can make the program even better.”
They found that there is a need for the supports to be extended as a transitional program in the community post-discharge, as the length of stay in the medical units tended to be short.
The project’s previous phase, involving acute and tertiary psychiatric care in the London region, prevented homelessness in 95 per cent of cases. “Going into the medical units, we found that people have highly complex needs that often involved mental health challenges.
By simply using the same approach that we did for those in psychiatric care, we helped half of the people find housing. To best serve the needs of everyone, we want to follow them after discharge.”
The team sees a solution in having a housing support worker provide transitional, wrap-around services that follow the person. They would continue to meet and work together after the hospital stay, helping to access community programs.
“This role would be embedded in both the health care system and the homeless serving system, supporting individuals who have complex physical and mental health issues as they are also navigating homeless resources.”
This project is funded by the Government of Canada's Homelessness Partnering Strategy’s (HPS) Innovative Solutions to Homelessness funding stream.
Overview and Numbers
Fast facts on homelessness and health care
- Stable housing after discharge is associated with higher quality of life, reduced substance abuse and fewer hospital admissions.
- Homeless clients are four times more likely to be readmitted to hospital within a month compared to low-income matched controls.
- Hospital care for homeless clients costs an average of $2,559 more per client.
- Finding appropriate housing or avoiding a potential eviction takes time – it is important to start as soon as possible during the discharge process.
Implementation of first phases of No Fixed Address
- Access on the unit to a housing advocate and income support staff.
- The initial intervention was accessed by 219 acute psychiatric clients, as well as 32 clients within a specialized tertiary care psychiatric hospital - only 3 became or remained homeless.
- Expanded to be an immediate wrap-around service with offices set up in the hospital mental health units.
- Staff from the Canadian Mental Health Association Middlesex (CMHA), Ontario Works (OW), and Salvation Army’s Housing Stability Bank (HSB) have on-site access to housing and income support databases.
- Clients can access service by drop-in or appointment.
- Services include assistance for finding housing, financial assistance, such as rent/utilities in arrears or first/last months’ rent for a new home, and access to high quality used furnishings, household supplies and a cleaning service.
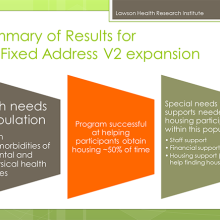
Expanded second phase of No Fixed Address
- Program ran from July 2018 to March 2019 (9 months).
- 74 people accessed the program.
- Complex situations with both mental health and physical problems: 100% had medical issues and 54% had mental health issues.
- Lengths of stay were very short.
- People could not attend drop-in due to medical issues, so they relied on referral from staff.
- Although they were all in imminent danger of homelessness, 38 people (50%) were housed as a result of this program.
Image
What were the main housing needs?
- Help finding a place to live
- Money for deposit
- Financial support
- Transportation support
- Help getting benefits
Recommendations and learnings for future models
Image
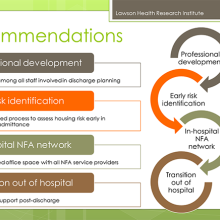
- Housing support worker needs to be a transitional support since work will be needed after discharge.
- Social work not the only key players (patient care facilitators, nursing staff, etc.).
- The transitional housing support role needs to be well embedded in the homeless serving system, as well as health care.
- People have physical and mental health issues and are also going to be navigating homeless resources.
- Despite the low success rate, many people were housed who would have otherwise been discharged to homelessness.
- We learned a lot about what was needed in an area where there was a knowledge vacuum.
- Future plans involve implementation with improvements to the model.
Scientist
Expanding transitional support for young adults with diabetes
In 2012, researchers from across Ontario, led by a team at Lawson Health Research Institute, started the first multicenter randomized controlled trial to evaluate implementation of a transition coordinator for young adults with type 1 diabetes as they transferred from paediatric to adult care.
“There is a huge difference between the kind of care that they receive as children compared to adults, and that is consistent across Canada and most other countries,” explains Dr. Cheril Clarson, associate scientist at Children’s Health Research Institute, a program of Lawson, and a paediatric endocrinologist at Children’s Hospital, London Health Sciences Centre.
With children, patient visits involve a variety of specialists from different areas, such as the physician, nurse educator, dietitian and social worker. “The naturally build up a long-term relationship with the team, as some children might start the program when they are 2 or 3 years old as an example.” Dr. Clarson adds that the child’s caregivers are an integral part of the process and the care team also gets to know them very well.
Moving into the adult program means that the patient now has more responsibility and autonomy over their own care. They have to remember to go to appointments, fill prescriptions and maintain their daily diabetes care.
“During the emerging adulthood period, your attention is taken up by many other things – leaving home, starting post-secondary education, figuring out your identity and independence,” says Dr. Tamara Spaic, Lawson associate scientist and adult endocrinologist at St. Joseph’s Health Care London. “And on top of that they need to manage their diabetes every day. They are in a completely new system with a new care team – it’s a major transition. For many, they stop coming to appointments regularly and they don’t keep up with all of their own care.”
As young adults struggle to find their footing in a new system, there are significant short and long-term consequences when it comes to their health. Some will experience acute complications like high sugars leading to diabetic ketoacidosis and hospital admission or severe low blood sugars where they can lose consciousness and have a seizure.
“Different studies show between 30 to 60 per cent increased risk of complications like retinopathy, myocardial infraction, stroke and kidney disease in those who do not follow their care plan,” notes Dr. Spaic. “We see a bump in this young adult period where levels spike and their diabetes isn’t being controlled – this has impacts for both the individual and the system.”
The study enrolled 205 young adults with type 1 diabetes between the ages of 17 and 20. Patients were recruited from three paediatric centres and their care was transitioned to three adult centres. The multi-centre partnership included Children’s Hospital; St. Joseph’s; Children’s Hospital of Eastern Ontario; The Ottawa Hospital; and, Trillium Health Partners in Mississauga.
Participants were randomly assigned to two groups, with 104 patients in the structured transition program and 101 patients receiving standard care. Patients were seen in the paediatric care setting for six months and then transferred to adult care, where they continued with either the transition program or standard care for one year.
The core component of the program was a transition coordinator, a nurse who is a certified diabetes educator. The coordinator followed the young adults throughout the transition, interacting with the paediatric health care team to establish a base of support as they moved into adult care. They attended visits, established appropriate contacts for the patient, provided support for diabetic care, problem solved and helped navigate the system. In addition to face-to-face meetings, they were available via text messages, emails and phones calls.
“We had a high recruitment rate for the population and type of study, and a high number of participants followed the full program,” says Dr. Clarson. “Our results at the end of the intervention showed that the program worked very well. By providing additional support through a transitional coordinator, the results showed better outcomes all around.”
Compared to the baseline, study participants attended more care visits, were more satisfied with their care, suffered much less distress associated with diabetes, had better management on a daily basis and reported less emotional burden of diabetes.
The team then took it a step further and spent another year following the participants to see if they were able to sustain the behaviour and positive outcomes. They did not find a difference between the control and intervention groups.
“Unfortunately, we found no difference in the number of visits they attended, their satisfaction with care and management of their diabetes,” explains Dr. Spaic. “When they didn’t have the intervention, they essentially went back to baseline. Out hope is to see the program extended.”
Dr. Clarson adds that they developed the program so that it can be integrated in different ways, and also in difference areas of health care beyond diabetes. For example, they found that the preferred method of communication with the coordinator was text. This is an easy way to provide the fundamental support of a coordinator for longer, and it is cost-effective.
“Our patients really loved the intervention. By the end of the study, they felt more comfortable being able to navigate the adult health care system. They felt empowered and responded well. They wanted to continue the program.” The next step for the researchers is to evaluate support through a virtual transition coordinator.
“Closing the Gap: Results of the Multicenter Canadian Randomized Controlled Trial of Structured Transition in Young Adults With Type 1 Diabetes” was recently published in the journal Diabetes Care by the American Diabetes Association.
Learn more about the study and read about Nicole Pelcz, study participant, who found out at 13 years old that she had type 1 diabetes.
In the media:
Diabetic teens fall back to old habits after transition care, study says – London Free Press
Scientist
August 11, 2022; Page 1 of 2 Low-Dose Naltrexone What is naltrexone? Naltrexone is an opioid antagonist, which means it blocks the effects of opioids such as codeine, morphine, oxycodone, etc. Naltrexone was developed to treat opioid addiction. A standard dose to treat opioid addiction is typicall...
… or perform excellent hand hygiene afterwards.) • Those planning to travel to areas requiring live vaccines; such as … be assessed by a travel medicine specialist for advice and planning and/or modify their travel plans. MEDICATION … or perform excellent hand hygiene afterwards.) • Those planning to travel to areas requiring live vaccines; such as …
CARING FOR THE BODY, MIND & SPIRIT SINCE 1869 Renowned for compassionate care, St. Joseph's is one of the best academic health care organizations in Canada dedicated to helping people live to their fullest by minimizing the effects of injury, disease and disability through excellence in care, teachi...
Page 1 of 2 February 16, 2023; Onabotulinumtoxin A (Botox) for Upper and Lower Limb Spasticity What is spasticity and how is it typically treated? Spasticity is a neuromuscular condition in which there is an abnormal increase in muscle tone, making the affected body parts stiff and difficult to move...
Page 1 of 2 February 16, 2023; Abobotulinumtoxin A (Dysport) for Upper and Lower Limb Spasticity What is spasticity and how is it typically treated? Spasticity is a neuromuscular condition in which there is an abnormal increase in muscle tone, making the affected body parts stiff and difficult to mo...
Page 1 of 2 February 16, 2023; Incobotulinumtoxin A (Xeomin) for Upper Limb Spasticity What is spasticity and how is it typically treated? Spasticity is a neuromuscular condition in which there is an abnormal increase in muscle tone, making the affected body parts stiff and difficult to move. Spasti...